Study Points
- Back to Course Home
- Participation Instructions
- Review the course material online or in print.
- Complete the course evaluation.
- Review your Transcript to view and print your Certificate of Completion. Your date of completion will be the date (Pacific Time) the course was electronically submitted for credit, with no exceptions. Partial credit is not available.
Study Points
Click on any objective to view test questions.
- Define the various conditions responsible for unintended weight loss in geriatric patients, including geriatric failure to thrive.
- Analyze various ethical and legal issues that can arise when treating geriatric failure to thrive patients and the role of advance directives in ameliorating some of these issues.
- Outline necessary components of the physical assessment and differential diagnosis of geriatric failure to thrive.
- Evaluate the role of polypharmacy in unintended weight loss in elderly patients.
- Describe the role of mental health screening in geriatric failure to thrive patients.
- Create a treatment plan for a geriatric failure to thrive patients, including possible pharmacotherapy approaches and areas for monitoring and follow-up.
- Identify geriatric failure to thrive patients for whom hospice referral should be considered.
Which of the following is NOT a chief characteristic of geriatric failure to thrive?
Click to ReviewFailure to thrive is defined by the Institute of Medicine as "weight loss of more than 5%, decreased appetite, poor nutrition, and physical inactivity, often associated with dehydration, depression, immune dysfunction, and low cholesterol" [6]. It is not a single disease or medical condition. Rather, it is a multidimensional problem that requires a multidisciplinary approach for its treatment. The four chief characteristics of geriatric failure to thrive are impaired physical function, malnutrition, depression, and cognitive impairment [7]. Failure to thrive is commonly used as a nonspecific diagnosis when a patient loses weight due to an unknown cause. After the diagnosis is made, it stimulates further assessment and interventions. Each of the domains of geriatric failure to thrive should be evaluated to determine areas in which the elder is having difficulty.
A male patient 78 years of age with COPD loses weight despite adequate nutritional intake. This is an example of
Click to ReviewCachexia is a physical wasting with weight and muscle mass loss, usually secondary to chronic progressive diseases such as cancer, acquired immune deficiency syndrome (AIDS), and chronic obstructive pulmonary disease (COPD). An estimated 10% of nursing home residents in the United States have cachexia [16]. Cachexia is a hypermetabolic state in which loss of body mass cannot be reversed nutritionally. The mechanisms that cause cachexia are poorly understood, but inflammatory cytokines and metabolic imbalances probably play a role [17,18]. Cachectic patients often have a poor prognosis due to multiple medical comorbidities. Cachexia is seen in the late stages of almost every major chronic illness, affecting an estimated 16% to 42% of people with heart failure, 30% of those with COPD, and up to 60% of people with kidney disease [18].
A patient with moderate cognitive impairment has no close family members. A close neighbor is designated to make his medical decisions. He is assigned to be the
Click to ReviewWhen caring for any patient with failure to thrive, it should first be determined if advance directives exist, and copies of any documents should be obtained. If no advance directives exist, it should be determined if the patient is capable of making his or her own healthcare decisions. This is called a determination of capacity and usually requires the signatures of two physicians. If the patient is deemed incapable of making medical decisions, the healthcare proxy will assume the role of medical decision maker. A healthcare proxy is a person that is chosen by the patient/family to make healthcare decisions for the patient. If there is not a surrogate designated, a close family member or personal friend may be appointed the proxy.
A woman who is 80 years of age has a living will that names her healthcare proxy. She also specifies that she does not want resuscitation or a feeding tube. The living will is activated when the patient
Click to ReviewThe concept of living wills grew from the limitations of DNR orders. These legal documents predetermine the medical care that will be accepted and refused. It may also designate a healthcare proxy or organ donation. If lifesaving or life-prolonging treatment is warranted and the patient is unable to communicate his or her preferences, the living will is activated. The living will should be as detailed as possible, and a physician should review the contents with the patient, if possible, to ensure understanding. A nutrition/hydration directive may be created in order to ensure that a patient's/proxy's wishes regarding nutrition and hydration care are followed. This clarifies whether a feeding tube may be inserted or IV fluids administered. In some cases, patients may refuse a gastric feeding tube but allow IV hydration or blood transfusion [22].
A gastric feeding tube is NOT an appropriate option for patients with which of the following conditions?
Click to ReviewGastric feeding tubes are commonly seen in nursing facilities, and they can be used for years to provide medications, hydration, and nutrition. Feeding tubes are routinely used for progressive neurologic diseases (e.g., Parkinson disease), stroke, and radiation therapy of the head or neck. However, gastric feeding tubes are not recommended for patients with advanced dementia, and there is no evidence that placement of a feeding tube improves the quality of life or survival in these patients [23,24]. Complications that can occur with a feeding tube include aspiration, infection, and tube dysfunction. In some cases, gastric feeding tubes prolong pain and suffering at the end of life. The impact of these potential complications should be considered before a gastric feeding tube is prescribed. Evidence-based information about feeding tube placement should be given to patients and family members to assist them to make informed decisions.
For patients at risk for malnutrition, dieticians would recommend
Click to ReviewDieticians perform nutritional assessments, recommend liquid supplements, discontinue restrictive diets, obtain calorie counts, determine food preferences, recommend protein supplements, and add nutritious snacks. Dieticians or dietary technicians should evaluate a patient's nutritional status regularly: upon admission to a nursing facility, quarterly, and in case of significant change in weight.
Which of the following is NOT a sign of dysphagia or aspiration?
Click to ReviewPatients often are at risk for aspiration secondary to dysphagia, and this complication is considered life-threatening. Therefore, patients with a diagnosis of dysphagia should be carefully monitored for signs of choking and/or pneumonia. Signs of dysphagia or aspiration include [31]:
Coughing or choking associated with eating
Excessive swallowing
Throat clearing
Gargling sound while eating
Wet voice
Sensation that something is stuck in throat
Food or liquid spilling from the mouth
Sneezing
Food pocketing in mouth
Recurrent pneumonia
Chest or lung congestion
Desaturation while eating
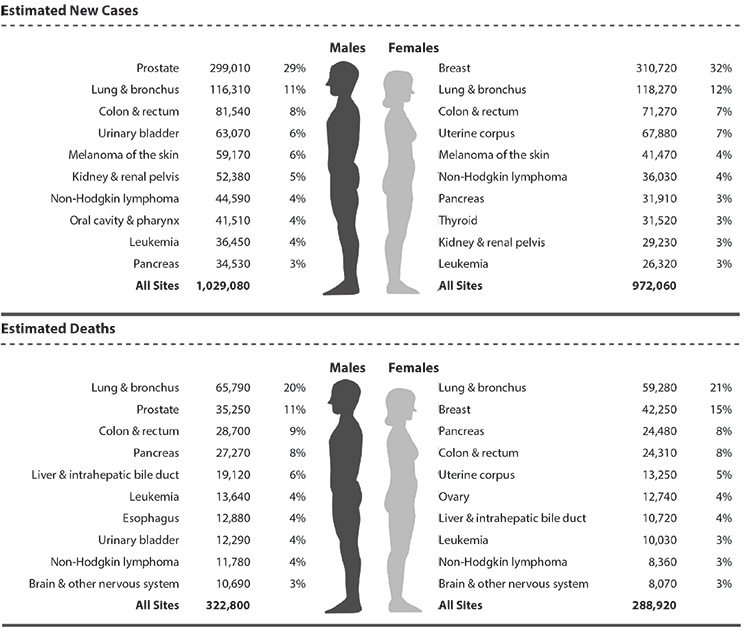
Which of the following is one of the top four cancers in the United States?
Click to ReviewWhich of the following is NOT a change associated with normal aging?
Click to ReviewA thorough baseline evaluation is necessary for all patients with unexplained weight loss. History taking and a complete and accurate physical assessment lay the foundation for further treatment, monitoring, and follow-up. A patient's baseline physical function and health should be determined before assessing for abnormalities. Changes associated with normal aging may include loss of subcutaneous fat from face and periphery (re-deposited to the abdomen and hips), shorter stature, shrinkage of muscle mass, kyphosis, and senile ptosis or ectropion. Many geriatric patients have chronic medical conditions, and seemingly abnormal exam findings may actually reflect these long-term illnesses (Table 1) [7]. Common findings in the geriatric patient may include heart murmurs and cardiac arrhythmias, chronic skin lesions such as seborrheic keratoses, orthostatic hypotension, sensory deficit (e.g. visual, hearing), and arthritic deformities. Good history taking with input from family members and staff will help differentiate problems that require intervention from normal findings for that patient. In addition to standard physical assessment, special attention should be paid to cancer detection, as discussed, and gastrointestinal tract disorders.
Which of the following medical conditions contributes to geriatric malnutrition?
Click to ReviewExamination of the abdomen may reveal hepatomegaly, masses, constipation, distention, hernias, ascites, and tenderness. Bowel and bladder patterns and function should be assessed, using the patient's normal patterns as a baseline. Conditions such as atrophic gastritis, gastric or peptic ulcer, constipation, lactose intolerance, diverticulosis, colitis, and diabetic gastroparesis may be the cause of significant weight loss. Diagnostic approaches for abnormal exam findings may include abdominal or pelvic ultrasounds, fecal occult blood test, and kidneys, ureters, and bladder x-ray. Referral to a gastroenterologist can be crucial for patients' treatment and outcome.
A patient with stroke and poor motor control of the right hand, which makes eating difficult, should have his or her functional ability evaluated by a
Click to ReviewImpaired physical function is one of the four domains of geriatric failure to thrive, and evaluation of physical functioning is an integral part of the geriatric evaluation [7]. It is important to determine any changes in mobility and evaluate for signs of a functional decline. This decline may be rapid, in cases of hospitalization and severe illness, or gradual, with the patient experiencing decreased mobility and independence over a period of time. Occupational therapists can provide a complete assessment of a patient's mobility and ability to perform activities of daily living (ADLs) and instrumental activities of daily living (IADL). The Katz ADL scale assesses six activities: bathing, dressing, toileting, transferring, continence, and eating [38,39]. The Lawton IADL scale assesses a patient's ability to use the telephone, shop, take transportation, manage a budget, adhere to medication regimens, cook, and perform housekeeping and laundry chores [40]. Approximately 34% of adults 65 years of age or older reported having some type of disability (i.e., difficulty in hearing, vision, cognition, ambulation, self-care, or independent living), and 49% of adults 75 years of age and older reported having difficulty in physical functioning. This ranged from 5% reporting it was very difficult (or impossible) to sit for two hours, to 33% reporting it was very difficult (or impossible) to stand for two hours [3]. For patients with failure to thrive, assessment of eating and ability to feed oneself is particularly important. Recommendations regarding contracture management and prevention, need for splints, positioning in wheelchairs or specialty chairs, and the need for assistive devices to help with eating may be made. A rehabilitation plan to assist the patient to regain independence in daily activities can be helpful.
Polypharmacy has been defined as the
Click to ReviewPolypharmacy has been described as the use of more than 5 medications, and excessive polypharmacy is defined as the use of more than 10 medications [43]. Known hazards of polypharmacy include lack of adherence, overtreatment, adverse drug reactions (including unexplained weight loss), and incorrect dose and administration regimen. In addition to these factors, physiologic changes of aging cause differences in the absorption, distribution, metabolism, and excretion of medications [44].
Which of the following medications is identified by the Beers list as a potentially inappropriate medication for the elderly patient?
Click to ReviewThe Beers list is a collection of medications potentially inappropriate for the elderly patient for a variety of reasons [45,46]. This list identifies medications not recommended for patients 65 years of age or older and identifies potentially harmful prescribing practices. Certain medications may be detrimental to elderly patients due to extended half-lives, interactions, or side effects. For example, benzodiazepines are associated with risk of cognitive impairment, delirium, falls, fractures, and motor vehicle accidents in the elderly, and before prescribing these medications, it should be clear that the potential benefits outweigh the risks [46]. Common medications on the Beers list include alprazolam, digoxin, cimetidine, diphenhydramine, lorazepam, and naproxen [45,46].
Which of the following medications is associated with falls in the elderly?
Click to ReviewMany patients take over-the-counter allergy, cold, or cough medications as sleeping aids, some of which contain acetaminophen/diphenhydramine. Elderly patients should be advised to avoid such use, as diphenhydramine is associated with falls in this population; another sleep aid can be prescribed [46,47]. Medications that patients have taken for years may require re-evaluation if changes in health status occur.
A score of 18 on the Mini-Mental State Examination indicates
Click to ReviewCognitive impairment is another domain of geriatric failure to thrive. To fully evaluate geriatric failure to thrive, it is necessary to also assess psychologic and sociologic functioning. The Mini-Mental State Examination (MMSE) or Folstein test may be used as an objective assessment of cognition, either to establish a baseline measurement of mental status or to track progress or decline [48]. It is a 30-item exam that takes approximately 10 to 15 minutes to complete. A correct answer for each item is awarded 1 point, and a score of 25 or more is considered normal. Lesser scores can indicate severe (≤9 points), moderate (10–20 points), or mild (21–24 points) cognitive impairment. It is helpful to document serial scores in the medical record.
A score of 3 on the Geriatric Depression Scale (short form) indicates
Click to ReviewThe Geriatric Depression Scale (GDS) is a self-report measure of depression that may be utilized to screen for depression in elderly patients (Figure 3) [7,54,55]. The shortened version (GDS-S) consists of 15 questions (taken from the long form) that assess mood and hopelessness. The GDS-S can be completed in five to seven minutes, which makes it ideal for patients who are easily fatigued or limited in their ability to concentrate for longer periods of time [55]. A score of 5 or greater on this test is considered positive. If a test is positive, referral to a psychiatrist specializing in geriatric patients should be made, as these patients do respond to depression treatment (e.g., psychotherapy, pharmacotherapy).
Upon evaluation of a geriatric patient with failure to thrive, the patient is noted to have a history of bipolar depression. She is prescribed several antipsychotic medications, one of which is suspected of causing the tremors that are making eating problematic. The next step is to
Click to ReviewThere are multiple long-term complications associated with typical and atypical antipsychotic medications, including pharmacokinetic and pharmacodynamic changes, limitations, and cardiovascular and other adverse effects (e.g., gastrointestinal, liver) [76]. A patient may develop a Parkinsonian syndrome secondary to long-term antipsychotic use, resulting in dysphagia, tremors, difficulty performing activities of daily living, and difficulty feeding, all of which can result in unintentional weight loss [76]. Prior to changing longstanding medication regimens, a geriatric psychiatrist should be consulted in order to help prevent exacerbation of the underlying psychiatric illness.
Which of the following medications is on the Beers list and should generally be avoided when treating geriatric weight loss?
Click to ReviewWhile megestrol has had some positive results for weight gain in the past, the potential drawbacks limit its use in practice. Patients with a history of thromboembolism should not receive megestrol. The Beers list includes megestrol acetate as a potentially harmful drug in the elderly, and its use should generally be avoided [81].
Megestrol acetate is specifically contraindicated in patients with a history of
Click to ReviewWhile megestrol has had some positive results for weight gain in the past, the potential drawbacks limit its use in practice. Patients with a history of thromboembolism should not receive megestrol. The Beers list includes megestrol acetate as a potentially harmful drug in the elderly, and its use should generally be avoided [81].
A geriatric patient with a BMI of 19.2 has continued to lose weight despite adequate treatment and is experiencing significant physical impairment. What should be strongly considered as the next step?
Click to ReviewDespite adequate evaluation and treatment, certain patients with failure to thrive will not respond to interventions. These patients will continue to lose weight and decline. If the BMI is less than 22 and significant physical impairment is causing disability, the patient qualifies for hospice care [91]. When the patient has declined parenteral feeding or has not responded to nutritional support despite adequate caloric intake, a referral to hospice should be considered. As noted, geriatric failure to thrive is no longer an acceptable diagnosis for hospice according to CMS [4]. Instead, the underlying condition most contributory to the patient's terminal prognosis should be noted (e.g., malnutrition).
- Back to Course Home
- Participation Instructions
- Review the course material online or in print.
- Complete the course evaluation.
- Review your Transcript to view and print your Certificate of Completion. Your date of completion will be the date (Pacific Time) the course was electronically submitted for credit, with no exceptions. Partial credit is not available.